
This post introduces two biological mechanisms believed to have contributed to the severity of the subject’s mTBI. On the balance of evidence, there is strong reason to believe that either, or both, of these injury modalities may play a significant role in the severity of mTBI injury, and therefore serve as contributing factors to the symptomology described as PCS.
The first section describes the subject’s work environment and his daily exposure to illumination. The second section provides a hypothesis regarding this level of illumination and its role in causing a deficiency in a neuro-protective factor. The third section also address the subject’s light exposure. It explores the degree to which this may have resulted in the deficient production of a hormone known to have both neuro-protective, and neuro-regenerative, properties.
The Subject’s Work Environment
The subject worked a permanent night shift starting work at 2030 hrs and completing work at 0700 hrs. This schedule had been followed for a period of 18 months prior to the March 6th, 2011 accident. The subject’s work schedule resulted in the complete reversal of his normal circadian rhythms. On return home in the morning, the subject was aware that any exposure to full daylight would make it impossible for him to enter sleep until late afternoon. Such delayed sleep would result in an abbreviated period of rest and high levels of fatigue during the following night shift. In order to meet the demands of his work schedule, the subject sought to be in bed, and asleep, by 0800.
The subject normally slept until 1700 or 1800, and then began preparations for his return to work. During the winter he would be exposed to domestic house lighting during this period. His bathroom receives no exterior illumination and all his windows face toward the east. During the winter months, the sun will have set by the time the subject wakes and enters the windowed living and dining area. The subject would drink a “morning” coffee but would delay any further meal until he arrived at work. Here he would make a fresh pot of coffee and consume two large cups at the start of his shift. He would snack at his desk until his first break at 2230, which break included another large cup of coffee and the final consumption of his snack. Approximately 2 hours later there was a “lunch” break at which time the subject consumed his major meal of the day. No further coffee or food was consumed after this time.
On completing the drive home, the subject would immediately retire, and avoid any activity, or stimuli, which might provoke him to stay awake. He believes his body was “fully trained” so that it would normally enter sleep between 0800 and 0830.
The workplace had been recently remodelled and conformed with the latest design trends for open office areas. The walls were painted a uniform bright white and all illumination was obtained from recessed ceiling fluorescent fixtures. There were no dimming controls available, and the lighting remained at full intensity throughout any 24 hour period. The subject’s seat faced east toward a large picture window approximately 50 feet from his desk which window gave a one third view of landscape shrubbery and a two thirds reveal of the sky. The subject had worked for the same firm for 12 years at a number of different locations and this last office was the brightest environment he had experienced in that 12 year period of employment.
The subject’s bedroom had a full height glazed patio door which gave access to an external balcony. The glazing gave an unobstructed view to the east. The window was covered by a series of vertical blinds. These served to screen out the daylight. During the winter at 45 degrees North latitude there is a greatly diminished level of solar radiation. It is possible to go for an extended period of days during which no direct sun is experienced.
The argument is made that the subject experienced two factors which had a bearing on the severity of his injury. Both of these factors are directly related to the levels of illumination experienced by the subject in the weeks and months prior to the March 6th, accident.
PCS Injury Modality 1 – Reduced UV Exposure
The subject’s daily routine in the weeks and months prior to the accident severely curtailed his exposure to UV light. UV light is known to be used by the pineal gland in the catalysis of heparin sulfate from biologically available sulphur derived from Brassicas, Alliums, and other foods.
The subject’s UV exposure was further curtailed by virtue of his latitude of residence and the presence of common winter conditions that greatly inhibited all solar illumination including both visible spectra, and UV.
It is therefore argued that the subject was UV deficient in the weeks and months prior to the March 6th accident and this fact greatly increased his risk of injury. Issues of UV exposure are described in detail in [NAME OF FUTURE POST]
PCS Injury Modality 2 – Functional Pinealectomy
It is known the avian pineal gland functions in a manner similar to that of the human suprachiasmatic nuclei. It has been shown by experiment with chickens that constant light exposure is equivalent to a functional pinealectomy.
It is argued that the subject’s work routine resulted in his exposure to near constant light. During the winter the subject would illuminate his house on waking with bright white incandescent bulbs (bedside lamp, dining, and kitchen area) or compact fluorescent bulbs (bathroom). There was no daylight exposure on waking as the sun had already set (On March 20th 2016, the vernal equinox, the sun will set at 1652 and rise at 0736). The subject would travel for 30 minutes in darkness to his brightly lit workplace and return home before the sun rose, or while it was still low to the horizon. By the time the sun had fully risen, the subject would normally be asleep. His bedroom was darkened by blinds but these show evidence of considerable light leakage on days of direct sunlight. It is not known to what degree human photo-receptors respond to indirect solar illumination.
Should human photo-receptors prove responsive to indirect solar illumination then, while the subject was asleep, the subject experienced a near constant diurnal cycle of illumination. This constant illumination would have compromised pineal production of melatonin. Since melatonin is understood to deliver significant neuro-protective benefit and neuro-regenerative benefit, this presumed melatonin deficiency would have increased the subject’s risk of brain injury and resulted in a diminished restorative response post injury.
These two factors of Reduced UV Exposure and Functional Pinealectomy would contribute to an increased severity of brain injury. The reduced neuro-regenerative benefit from melatonin deficiency likely prolonged the injury, inhibited restoration and contributed to the symptomology described in the International Classification of Diseases (ICD-10) diagnostic criteria for Post Concussion Syndrome (PCS).
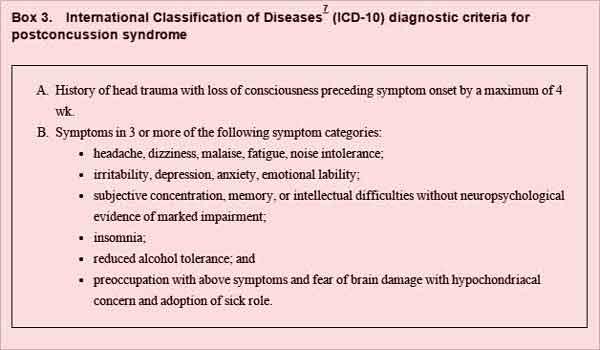
Figure 3 – ICD 10 Diagnostic Criteria for PCS
Can Fam Physician. 2012 Mar; 58(3): 258.
—————————————
A Note on the Header Image
The header image was taken at 1110 hours on January 19th, 2016 and is representative of the dull winter illumination present during the winter at 45 North latitude.
Posts in the PCS Sequence
PCS Thesis – Index
PCS Thesis – The Accident
PCS Thesis – The Pineal Gland
PCS Thesis – UV Index